
When MRI Abnormalities Are Not Abnormal: "Age-Appropriate" Changes Found in 95% of Shoulders.
Your MRI report doesn't matter nearly as much as you might think

I have been saying this for more than fifteen years, long before it was even comfortable to say out loud: very little of what we see on an MRI explains pain. The pain research in this respect has been clear for a long while. Imaging findings rarely correlate well with symptoms.
When I first started practicing, imaging and their reports felt definitive. A rotator cuff tear, a labral tear, a meniscus tear, femoroacetabular impingement—those words carried authority... and were often followed by a scheduled surgery. These findings sounded structural and mechanical, and by extension, fixable. Surely somethings that’s broken needs to be fixed. Nope.
Over time, though, something did not add up. I kept seeing patients whose imaging looked horrible but who functioned really well, and others whose scans looked modest but who were limited and uncomfortable. The mismatch was too consistent and couldn’t be dismissed as coincidence.

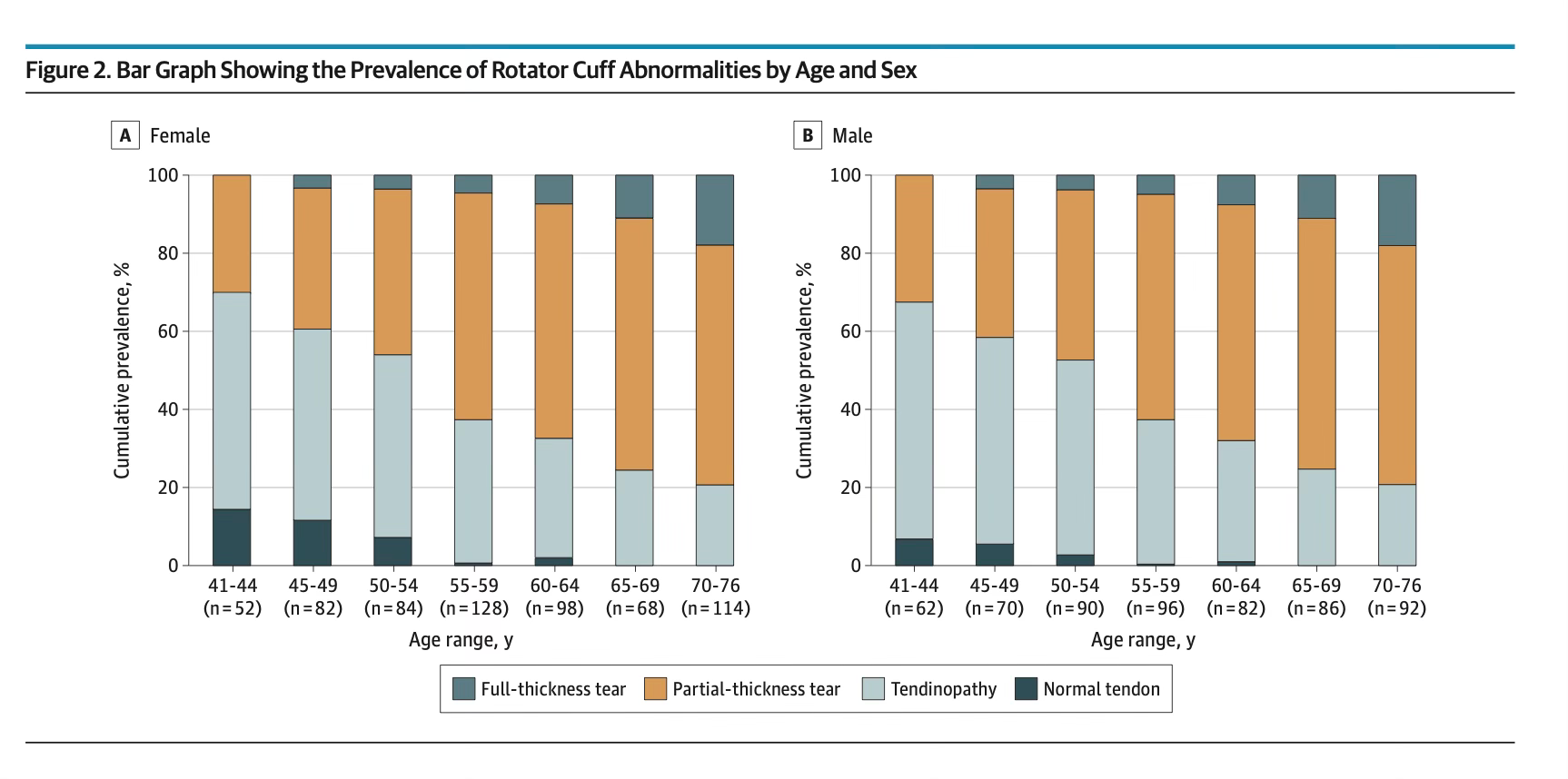
Now the imaging data are catching up to what some of us have observed clinically. A recent population-based MRI study published in JAMA Internal Medicine scanned more than six hundred adults between the ages of forty-one and seventy-six, regardless of whether they had shoulder pain.
Nearly ninety-nine percent had some rotator cuff abnormality on MRI . Tendinopathy, partial-thickness tears, and even full-thickness tears were almost universal findings as people aged (see the graph below). What was more striking was that these abnormalities were just as common in people without symptoms as in those with pain. Even full-thickness tears, which instinctively feel like they should all hurt, lost their association with symptoms once the analysis accounted for other clinical variables .
In practical terms, that means a substantial percentage of what we label as pathology may simply represent normal age-related change.
I’ve written extensively about age-appropriate changes - search this site or my old website for that term. The concept isn’t new, but the problem persists (and will persist) as long as medicine is driven by productivity, procedural volume and some surgeons who measure success by surgical volume.
The challenge is determining who actually needs surgery. Many rotator cuff tears do fine without surgery - partial tears especially. Tendon pain from metabolic disease (which I’ve discussed often here) won’t easily show up on imaging studies. Yet the imaging abnormality often drives the surgical recommendation.

But why do some people not have pain, or some improve with PT, yet others remain miserable? Sometimes people don’t respond to injections and physical therapy and go on to surgery… but that should be a very small number. We operate on far too many people today, and many surgeries are indicated for imaging findings alone. Often the reason you don’t respond isn’t the “tear” but it’s your overall health. Metabolic disease is associated with inflammation. That can make it much harder to resolved a painful tendon issue. It also requires a different approach.
Another issue, this imaging pattern is not confined to the shoulder. We have seen it in the spine, where disc bulges and herniations are common in people who have never had back pain. Nearly 100% of adults have a disc abnormality. So, when you get into a car accident and blame the accident for your disc problem… think again. Yes, something hurts… but it’s probably not what the MRI shows.
We have also seen this with degenerative meniscus tears in middle-aged adults, where imaging often reflects tissue aging rather than a mechanical injury that requires repair. We see it with many hip labral tears and with the bony morphology labeled as femoroacetabular impingement. Structural changes accumulate with time. You don’t still drive your first car… do you? Why do you think your MRI should say normal shoulder after 50 years of use? They are part of living in a body. The presence of an abnormality on imaging does not automatically establish causation.
The challenge is not only scientific but psychological. This is a problem we face in the office every day. The words we use—tear, degeneration, damage—carry emotional weight. Patients hear those terms and understandably assume something is broken. Once that belief takes hold, fear and avoidance often follow. When nearly everyone over forty has some degree of rotator cuff abnormality , the presence of a tear alone cannot be treated as proof of disease, or pain. This is where the LLMs and robots will falter.
The Power of Listening, Reassurance, and the Right Conversation
Sometimes, the most powerful thing we can say to a patient is:
The more meaningful question is whether the clinical story, examination findings, and functional limitations align in a coherent way. This is key. We’ve become a high tech, low touch healthcare system where objective data (imaging) is given priority over a proper history and exam. If you don’t listen to your patients, and examine them each time, you’re going to miss something. And you’re very often going to miss the right diagnosis.
High-Tech and Low-Touch Medicine: Navigating the Future of Human-Centered Healthcare

A paradox emerges in the evolving landscape of modern healthcare: as technology advances, the traditional human-centered aspects of medicine, such as the art of physical examination, are diminishing. This shift towards a high-tech, low-touch approach raises profound questions about the future of healthcare and the role of physicians. Simultaneously, doc…
Here is the foundation of a message I have been repeating for decades: you are not broken. Aging tissues adapt and remodel. They accumulate structural changes that look dramatic on a screen or report but often function remarkably well in real life. When we frame every structural variation as pathology, we risk overdiagnosis and overtreatment. When we instead recognize that many imaging findings are common, or age-related phenomena, we can shift the focus back to capacity, strength, load tolerance, and resilience.
None of this implies that imaging is irrelevant or that surgery is never appropriate. There are clearly situations where structural pathology and symptoms align, and intervention improves quality of life. The point is that imaging must live in context. It is one piece of information in a larger clinical puzzle. A longevity-oriented approach to musculoskeletal care depends on this perspective. If we treat every scan as evidence of failure, we medicalize normal aging. If we treat people instead of pictures, we preserve function and confidence.
For more than a decade and a half, I have told patients that their MRI is not their identity. Increasingly, high-quality population data support that stance. The real work is not in fixing every abnormal image but in helping people build durable, adaptable bodies that tolerate load and continue to move well for decades. That philosophy begins with a simple but often countercultural premise: structural change does not equal structural catastrophe… and if you’re ever told you need orthopedic surgery due to an MRI finding… get a few more opinions.
I trust I wasn't too harsh here…
Thanks for this. It's such a challenge, keeping up a strong functional body as one gets older. I've researched what seems to be appropriate PT as I wait for both a doctor and PT appointment for what seems obvious to be a shoulder tear. Fortunately I am overall quite healthy. Glucose allways low. Last insulin was not as recent but was very low. I am finding your education on this subject very helpful. Thank you much.
My imaginary showed a full thickness tear in my supraspinatus 9 yrs ago and was told I needed surgery, I kept working out and went to physical therapy for 6 months and have had no trouble since. At the time it was very painful.