
BEFORE THE INCISION: Preparing for Elective Surgery
The operation is 45 minutes. The recovery is months. What you do before surgery matters far more than you think.

I have performed thousands of surgeries over 30 years… and I can’t stress this enough: The patients who do best after surgery are not the ones with the ‘best’ surgeon or the most recent implant design. They are the ones who showed up ‘prepared’. Physically strong, metabolically healthy, mentally ready, and adequately informed about what was coming.
I have watched patients struggle through recoveries that were harder than they needed to be, but not because the surgery went poorly. Instead, it was because they were not ready for it. They were deconditioned, had significant systemic inflammation, anemia, poorly controlled diabetes, abdominal obesity, or were simply unaware of what the rehabilitation would demand. Some of those patients should not have had the surgery at that time. They needed to get stronger and healthier first. I know that this sounds exclusionary… but it’s best to avoid the right operation on the wrong person. Otherwise, they could be worse off than they were before the surgery.
This post is about everything that happens before the incision. It is long, and it covers a lot of ground. It also has a section written by one of the best anesthesiologists I’ve ever worked with. If you or someone you care about is having elective surgery, this is the information you need to know… regardless of the procedure. The definition of a ‘small procedure’ is one performed on someone else.
For Members, there will be a downloadable guide at the very end.
You should probably have a second opinion.
I know that’s an uncomfortable question to hear from a surgeon. But this is the right place to start. I don’t agree with nearly as many second- or third-opinion cases as I did in the past. It could be that the patient wasn’t ready, or simply that the surgery wasn’t indicated.
Elective surgery means the procedure is scheduled, not emergent. You have time. And that time should include ensuring the operation is truly indicated and that you’ve exhausted non-surgical options first.
The data on second opinions is not surprising to me. Studies on mandatory second-opinion programs for elective surgery report disagreement rates of 20-40%. That means, in roughly one out of every three to five cases, a second surgeon examined the same patient and said, “I wouldn’t operate.” In one orthopedic study, 82 percent of patients who were told by a second consultant that surgery wasn’t necessary had still not had the operation six months later, and they were doing fine. The most common reasons for non-confirmation were that non-surgical treatment was preferable, symptoms weren’t severe enough, or physical therapy hadn’t been adequately tried.
The more recent second-opinion data warrant further discussion, particularly in spine and knee surgery. A 2021 Bavarian insurance program that required second opinions before knee replacement found that only 40 percent of initial surgical recommendations were confirmed by a second surgeon. Another 40 percent were told the surgery might be appropriate later but was not indicated yet, and 20 percent were told it was not indicated at all.
In spine surgery, the numbers are consistently worse. A scoping review of 14 studies published in Surgical Neurology International in 2021 found that 61 percent of spine surgery second opinions were discordant, with three out of four of those recommending conservative management instead.
A large Spanish second-opinion program tracked over 1,000 spine surgery referrals over eight years and found that 61 percent of patients were redirected to conservative treatment after review, resulting in improved outcomes and significant cost savings.
These studies reflect a consistent pattern across multiple countries, insurance systems, and surgical specialties. The reasons for non-confirmation are almost always the same... non-surgical treatment had not been adequately tried, symptoms did not match the imaging findings, or the structural changes on the scan were age-appropriate and not the actual source of the problem.
None of this means surgery is never the right answer. It means that for elective procedures, a second set of eyes is one of the most valuable things you can get before making that decision.
I’m a surgeon, and I am not anti-surgery. But I have spent 20+ years watching imaging finding alone drive decisions that should have been driven by pain and/or loss of function. An MRI that shows a meniscus tear, a labral tear, a disc bulge, or cartilage thinning reveals a condition common in pain-free adults over 50. In imaging studies of pain-free adults with no symptoms, a very large percentage of knees show at least one abnormality on MRI. 90+% of people over 40 have a rotator cuff ‘abnormality’ on MRI. Many of these are normal age-related findings. They are not, by themselves, a reason to operate.
The questions that should drive the surgical decision are functional:
Does this problem significantly limit what you can do in daily life?
Does the pain significantly impact your quality of life?
Have you given non-surgical management, physical therapy, load modification, injections, time, a long chance at working?
Is your surgeon recommending surgery because of what you can’t do, or because of what the scan shows?
If you haven’t gotten a second opinion, consider one. For most elective orthopedic surgery, if you haven’t tried physical therapy for at least 8 to 12 weeks with a therapist who understands progressive loading, do that first.
If the surgery is truly indicated, it will still be indicated in two months. And you’ll be stronger and more prepared for it.
Are you ready for this surgery?
This is a different question from whether you need it. I see patients in my office regularly who have a clear surgical indication. Their pain is real. Their imaging correlates with their symptoms. The surgery makes sense. But from my assessment, they are not ready.
The right operation on the wrong person is a recipe for disaster.
They’ve lost so much muscle mass and strength over the years that they can barely get out of a chair. Their aerobic fitness is very poor. They’re carrying 40 or 50 extra pounds, much of it visceral (inflammtory) fat. Their Hemoglobin A1c is 8.2. They’re on four blood pressure medications, rarely take them, and their blood pressure is poorly controlled. They haven’t exercised in years. They can’t climb a flight of stairs without stopping due to shortness of breath. These are all warning signs. They’re not absolute contraindications. I’ve done knee replacements on people in their 90s who have sailed through… and I’ve avoided operating on some people in their 60s, because they would not have. Age is a very relative factor in this decision-making.
If I operate on the ‘wrong’ patient, the surgery itself might go perfectly. But the recovery will be brutal. They won’t have the strength to do the rehab. They won’t have the cardiovascular reserve to tolerate the physical therapy sessions. They’ll be at higher risk for blood clots, infection, wound complications, and prolonged hospitalization. The outcome could be worse than it should be, not because of the operation, but because the body receiving it wasn’t prepared.
The operation is 45 minutes. The recovery could take 4-12 months. Surgeons and patients are a team. But the patient is doing more of the work on this team. Recovery is the hardest part, and a significant part of the recovery depends on what you bring into the operating room.
I can assure you that your recovery could possibly take twice as long as you expect.
If your surgeon tells you that you need to get healthier before surgery, please take that seriously. A knee replacement in a patient with an A1c of 6.5, strong quads, and the ability to walk a mile is fundamentally different from the same operation in a patient with an A1c of 8, significant muscle loss, and the inability to stand from a low chair.
Metabolic optimization
Your metabolic health directly affects your surgical risk, your healing, and your recovery. These are measurable and modifiable variables with strong evidence behind them.
Hemoglobin A1c and blood sugar. If you have diabetes or prediabetes, your A1c should be below 7.5 (the AAOS says 8) before elective surgery, and ideally below 7.0. For every unit increase in A1c, the risk of surgical site infection, wound complications, and postoperative mortality climbs. Poor glucose control slows wound healing, impairs immune function, and increases the risk of prosthetic joint infection, which is a devastating complication. It also diminishes the chance that your tendon repair will heal.
Work with your primary care physician or endocrinologist to optimize your glucose control in the months leading up to surgery. This is not something to address the week before the operation.
Anemia. A significant percentage of patients presenting for elective surgery are anemic. The most common cause is iron deficiency, which is treatable. Preoperative anemia increases the risk of blood transfusion, postoperative complications, and longer hospital stays. If you are having elective surgery, ask for a complete blood count and iron studies well in advance. If you’re iron-deficient, there is time to correct it, either with red meat, oral iron (which takes weeks), or intravenous iron (which works faster). You don’t want to start a major operation already short on the oxygen-carrying capacity you’ll need for healing.
Blood pressure. Uncontrolled hypertension increases perioperative cardiac risk. If your blood pressure is consistently above 160/100, most anesthesiologists will want it optimized before proceeding with elective surgery. Don’t wait until the pre-op visit to discover this. Monitor your blood pressure at home in the weeks before surgery and work with your physician to get it under control.
Weight and body composition. I am not going to give you a BMI cutoff and tell you that you can’t have surgery above it. But I will tell you that excess visceral fat increases systemic inflammation, worsens insulin resistance, could make surgical access more difficult, increases wound complication rates, and makes rehabilitation harder. If you have months before your surgery, losing even 10 to 15 pounds of visceral fat can meaningfully improve your metabolic profile and your surgical risk. The goal isn’t a number on the scale. The goal is to reduce the structural, inflammatory, and metabolic burden your body carries into the operating room.
Smoking. Stop. Full stop. Smoking is the single strongest modifiable risk factor for wound complications, infection, and poor bone healing. It impairs oxygen delivery to healing tissues, constricts blood vessels, and compromises immune function. If you cannot quit permanently, quit for at least 4 to 6 weeks before surgery and 4 to 6 weeks after. Your surgeon and anesthesiologist will both be more comfortable operating on you, and your tissues will heal better.
Alcohol. Heavy alcohol use increases bleeding risk, impairs liver function (which affects how you metabolize anesthetic drugs), disrupts sleep, and weakens immune response. If you drink more than moderately, cut back well before surgery. If you drink heavily, your anesthesiologist needs to know because alcohol withdrawal in the perioperative period is dangerous.
Physical preparation: Prehabilitation
Prehab is the most underutilized tool in elective surgery. The concept is simple: get yourself as strong, fit, and functional as possible before the operation so you can start recovery from a higher baseline.
The evidence supporting prehab exists. ERAS (Enhanced Recovery After Surgery) protocols, which have become the standard of care for many surgical specialties, include structured preoperative exercise as a core component. Studies consistently show that patients who engage in prehabilitation have fewer complications, shorter hospital stays, less pain, and faster return to function.
What does prehab actually look like? It depends on your surgery and your starting point, but the principles are consistent:
Strength. If you are having lower extremity surgery, your quadriceps, hamstrings, glutes, and calves all matter. Upper body strength matters, too, because you’ll use your arms to get out of bed, off the toilet, and up from a chair with crutches or a walker. If you’re having upper-extremity surgery, your core and lower-body strength will carry you through the early recovery. The point is that strength is an important systemic variable. You don’t just need the muscles around the surgical site. You need the whole system to function more efficiently.
Aerobic capacity. Surgery is a physiological stress test. Your heart, lungs, and cardiovascular system need the reserve to handle anesthesia, blood loss, pain, medications, and the metabolic demands of healing. Walking, cycling, swimming, or any sustained activity that elevates your heart rate for 30 to 45 minutes most days will build the reserve you need. Even 4 to 6 weeks of consistent aerobic work before surgery makes a measurable difference.
Balance. If you’re having lower extremity surgery, you will be on one leg, with a walker or crutches, navigating stairs, stepping over thresholds, and managing uneven surfaces while you recover. If your balance is poor going in, your fall risk after surgery is high. Single-leg stance practice, tandem walking, and step-ups are simple and effective.
Protein. Your body needs raw materials to heal. Protein requirements go up before and after surgery, not down. Aim for 1.2 to 1.6 grams of protein per kilogram of body weight per day in the weeks leading up to surgery, distributed across 3 to 4 meals with 30 to 40 grams per meal. This is the same recommendation I make for midlife athletes, and it applies here for the same reason: you need to overcome anabolic resistance and reach the leucine threshold to maximally stimulate muscle protein synthesis. Healing tissue is hungry tissue.
Check your vitamin D level and bring it above 30 ng/mL. Consider collagen peptides and vitamin C for connective tissue support. Creatine monohydrate (5 grams per day) can help preserve muscle mass during the post-surgery period of reduced activity.
Do not go on a caloric deficit before surgery. Now is not the time to lose weight through restriction. You need adequate energy to build strength, support immune function, and prepare for the stress of the operation. If weight loss is part of the plan, it should happen in the months before prehab begins, not during it.
From the Anesthesiologist’s Perspective:
A guest perspective by Dr. Jonathan Bauman: Jon was one of the finest anesthesiologists I have ever worked with across my 25-year career.
Let me tell you what I actually do for a living.
Most people picture the anesthesiologist as the person who puts you to sleep and wakes you up. You meet me for about 5 minutes before the operation, I ask you a bunch of questions – most of which you’ve been asked before –, and before you know it, the surgery is done. You’ll probably see me once more, but chances are, you won’t remember that.
Here’s what that looks like from my side: I’ve spent years training to manage the most dangerous minutes of your surgical experience. The surgeon is focused on the joint, the hernia, the tumor — their world is eight inches wide and entirely in front of them. My world is your entire body, all at once, for the duration. Heart rhythm, blood pressure, oxygen, breathing, temperature, fluid status, and anesthetic depth — simultaneously — while providing the surgeon with optimal operating conditions.
Anesthesia is often compared to flying a plane: hours of boredom, moments of terror. When done correctly, anesthesia should never be boring (constantly monitoring everything mentioned above and more is not boring at all), and moments of terror should be once in a blue moon.
That’s why I ask so many questions.
What I’m Actually Learning When I Ask
When I do your preoperative assessment, I’m building a risk profile. The questions that seem redundant to you are not redundant to me.
“How many flights of stairs can you climb?” — This lets me know how well your heart functions. If you can’t go up a flight of stairs, I need to understand why. Is it because your knee hurts after a couple of stairs, or do you become too short of breath to continue?
“Do you snore? Has anyone told you that you stop breathing at night?” — This helps me assess obstructive sleep apnea risk. It means a potentially difficult airway (hard to put a breathing tube in), high sensitivity to postoperative opioids, and elevated breathing risk, especially after the surgery.
“Have you or any blood relative ever had a problem with anesthesia?” — This asks about a disease unique to anesthesia and 2 types of medications we frequently use—inhaled anesthetics and depolarizing muscle relaxants (you don’t have to remember either)—malignant hyperthermia (MH). MH is a rare, inherited, life-threatening reaction. The nice thing is that if I know about it, I can do things to prevent it and provide a safe anesthetic for your surgery.
“Open your mouth wide. Stick your tongue out.” — I’m scoring your airway to assess how easy or hard it might be to place a breathing tube if necessary for the operation. A difficult airway changes my equipment, my setup, and sometimes my entire anesthetic plan.
“When did you last have anything to eat or drink?” — One of my main concerns when you go to sleep is something called an aspiration. That’s when stomach contents come up from your stomach and end up in your lungs. Also rare, this can be catastrophic. By asking this question, I can minimize your risk of aspiration.
The above are a sample of questions that have the greatest impact on ensuring you have the safest possible surgery and anesthetic. There are many other questions I’ll ask before your surgery to ensure I have a complete understanding of your medical history and surgical/anesthetic risks. These aren’t bureaucratic checkboxes. Each one is telling me something specific about your risk.
The Anesthesia Conversation You Didn’t Know You Could Have
Most patients assume they’ll be “put to sleep” and that’s the end of it. It isn’t.
General Anesthesia: This is typically what people refer to as “going to sleep.” Although it comes with some risk and may increase the incidence of certain post-operative side effects like nausea and vomiting, sore throat, and dental injuries, general anesthesia is sometimes the only appropriate choice. There is an increasingly recognized risk in people over 65 years old of postoperative neurocognitive disorders that can range from temporary postoperative delirium to something more persistent. Despite what I wrote above, general anesthesia is still exceeding safe.
Spinal or Epidural Anesthesia: For many orthopedic procedures and surgeries below the waist, spinal/epidural anesthesia typically offers a better recovery profile — less nausea and vomiting, sore throat, and dental injuries. People tend to “feel better” after this type of anesthesia compared to general anesthesia. Because a spinal/epidural requires me to put a needle in your back near your spinal cord, I am frequently asked, “Can’t I become paralyzed from the spinal?” When placing a spinal, my needle is actually far enough away from your actual spinal cord that the risk of paralysis is close to zero (nothing in medicine is zero). To give you an idea of how safe a spinal is, I had one when Howard operated on me.
Peripheral nerve blocks: Similar to a spinal anesthetic that blocks the nerves in the central nervous system (spinal cord) with local anesthesia, peripheral nerve blocks block the nerves that go to your limbs. These have transformed postoperative pain for orthopedic patients. By injecting local anesthesia around the nerves that go to your arm or leg, I can, in certain cases, provide Howard with such good surgical conditions that his patients can otherwise be wide awake during the surgery - don’t worry, I’ll sedate you for the operation so you don’t know what’s going on. Waking up from surgery without the searing pain that used to be the default experience is now achievable and expected in high-quality programs.
Don’t be afraid to ask your anesthesiologist which type of anesthetic or combination is best for you and the type of surgery you’re having. You can always request a specific anesthetic, but keep in mind that, ultimately, the decision should be a joint one, made through a conversation among you, your surgeon, and an anesthesiologist.
Medications That Can Cause Problems
GLP-1 agonists — These medications have become ubiquitous over the last few years because of the myriad health benefits they provide. Common examples include semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro). One of the few areas where these medications cause concern is in the operating room with anesthesia. The reason is that one mechanism that causes weight loss is slowing the emptying of your stomach, so you feel full. Having a full stomach increases your risk for aspiration (see above). It was originally thought that the injectable medications should be held for 1 week prior to surgery. Recent data, however, suggests that people should continue these medications throughout the pre-operative period. Please follow your surgeon's or the perioperative nursing staff's recommendations before your surgery. Each site may have different medication instructions.
SGLT2 inhibitors — These medications are on the rise, as well. They not only help people with Type 2 diabetes control their blood sugar but also offer heart and kidney protection in some patients. Examples are empagliflozin (Jardiance), dapagliflozin (Farxiga), and canagliflozin (Invokana). These medications can cause something called euglycemic diabetic ketoacidosis in the perioperative period. It’s not worth getting into what that is, but it can cause significant complications for otherwise very safe surgeries. These medications should be held for 3-4 days prior to your surgery.
Anticoagulants (blood thinners) — Management of these medications pre-operatively requires careful hold-time decisions that often involve clinical input from your cardiologist, surgeon, and anesthesiologist.
Supplements: fish oil, vitamin E, ginkgo, garlic, NSAIDs (Advil, Motrin, aspirin, etc.) — these affect platelet function and bleeding. Some should be held before surgery, others shouldn’t. Please let us know all the supplements and over-the-counter medications you are taking. Most are very safe to continue; others can affect your surgery and outcomes.
What I Wish You’d Do Before You Showed Up
Know your medications by name and dose. “The little white one” doesn’t help me.
Tell me your anesthesia history — yours and your blood relatives’. If you woke up vomiting for hours after a previous surgery, I’d like to know that so I can prevent it from happening again.
If you’re on a GLP-1 or SGLT2 inhibitor, proactively ask your prescribing physician or surgeon about perioperative hold guidance before your surgery date.
Optimize what you can control — blood pressure, blood sugar, smoking. These aren’t arbitrary requests; each genuinely changes your risk. This is where a good primary care physician is invaluable.
And be honest with me. I’m not here to judge you about your drinking, your weight, your missed medications, or your anxiety. I’m here to keep you safe and make sure you have the best surgical experience possible. The more accurately I know your health picture, the better I can do that job. The more you tell me, the better.
2 Words I Hope To Never Hear Again
“Medical Clearance”: You are not alone. I hear patients, surgeons, internists, nurses, and even anesthesiologists ask about medical clearance before surgery. Medical clearance implies permission for you, the patient, to have surgery. The only 2 people who actually clear the patient for surgery are the surgeon and the anesthesiologist. Sometimes we do need help from a primary care physician, cardiologist, pulmonologist, etc., to determine if you are medically optimized for the surgery. In other words, are you in the best medical condition possible before coming to the OR? That’s where a medical evaluation comes in handy.
Believe it or not, the majority of patients who come through our operating rooms don’t need a medical evaluation from a primary care physician or specialist before their surgery.
The same goes for labs and additional testing, such as EKGs and stress tests. The days of patients being cleared and having routine pre-operative testing labs, chest x-rays, EKGs, etc., are over. Just like your healthcare is tailored to you, so is your pre-operative work-up.
Mental preparation and setting expectations
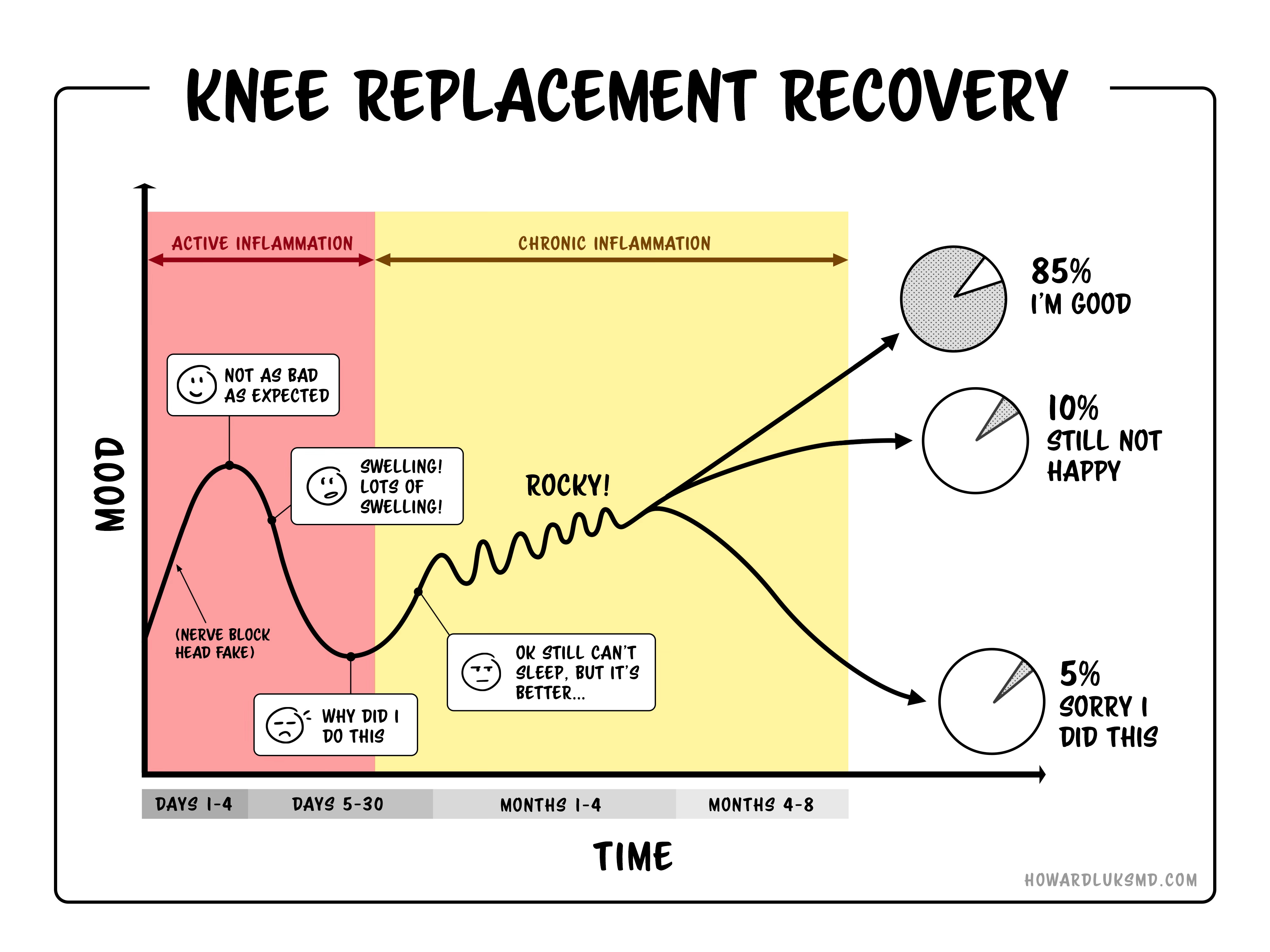
Recovery from major surgery is long, hard work. It takes effort, patience, and persistence. There will be days when swelling and stiffness slow you down, when progress stalls, when you wonder whether the surgery was worth it. That is normal. Nearly every patient I’ve operated on has had those days. I give the diagram below to every patient undergoing a knee replacement. Look at day 5.
The patients who do best are the ones who go in with realistic expectations. A knee replacement is not a reset button that makes your knee 25 years old again overnight. A rotator cuff repair does not give you a brand new shoulder. Surgery restores function within the limits of your biology, your effort, and your starting point. The operation can replace a joint or repair a structure. It cannot restore strength, coordination, or metabolic resilience. Those have to be earned through preparation and postoperative rehabilitation. If you have an A1c over 7 and an elevated CRP indicative of systemic inflammation, you’re going to have a more stormy post-operative course. You should be prepared for that. Furthermore, you may have an incomplete recovery, with results falling short of your expectations.
Set specific, achievable milestones. Walking around the house without a walker. Climbing a flight of stairs. Driving again. Returning to your exercise routine. These create steady forward progress and a sense of accomplishment. They also prevent you from falling into the trap of comparing your timeline to someone else’s. Your neighbor, who was hiking 6 weeks after a knee replacement, could have had a different body, lower inflammation, and different pain tolerance than you. Your recovery is your own.
One thing I tell every patient: the people who struggle are often the ones who stop moving once surgery is on the calendar. They think rest will protect their joint, their shoulder, or their spine. In most cases, the opposite is true. Every day before surgery is an opportunity to get stronger. Please do not waste it.
The week before and the day of…
Two weeks before: Contact your surgeon’s office and confirm your preoperative checklist. This typically includes preoperative labs (blood count, metabolic panel, coagulation studies), an EKG if indicated, and a medical evaluation from your primary care physician or cardiologist if you have a cardiac history. Confirm which medications to stop and when to stop them. Get your prescriptions for post-surgical medications filled in advance so they’re waiting at home when you get back.
One week before: Set up your home for recovery. If your bedroom is upstairs and your surgery is on a lower extremity, consider sleeping downstairs for the first few weeks. Install grab bars in the bathroom if needed. Stock your kitchen with high-protein, easy-to-prepare meals. Freeze some meals in advance. Get a reacher/grabber if you’re having hip or knee surgery. Remove throw rugs and tripping hazards. Charge your devices. Have ice packs ready.
If you’ve been prescribed a preoperative skin preparation (antiseptic wipes or wash), use it as directed in the days before surgery. This can reduce the bacterial load on your skin and lower your risk of infection.
The night before: Follow your surgeon’s and anesthesiologist’s instructions on eating and drinking. The standard is no food after midnight, though some ERAS protocols now allow clear liquids up to 2 hours before surgery, with a carbohydrate-containing drink. Follow whatever instructions you are given, not what you find on the internet.
Lay out loose, comfortable clothing that you can get into easily after surgery. If you’re having shoulder surgery, wear a button-down shirt. If you’re having knee or hip surgery, wear loose shorts or elastic-waist pants. You’ll definitely prefer slip-on shoes.
The day of: Arrive on time. Bring your ID, insurance information, and a list of your current medications and dosages. Leave jewelry, valuables, and contact lenses at home. Have a responsible adult ready to drive you home and stay with you for at least the first 24 hours.
You will likely meet your anesthesiologist that morning. This is your chance to ask questions about anesthesia type, pain management, nausea prevention, and anything else that concerns you. Do not be shy. They want you to be informed and comfortable.
Take-home points
Get a second opinion. If the surgery is truly indicated, a second surgeon will confirm it. If it isn’t, you’ve saved yourself a major operation.
Being indicated for surgery and being optimized for surgery are two different things. If your A1c is elevated, your blood pressure is uncontrolled, you’re severely deconditioned, or you’re anemic, get those issues addressed first. The surgery will still be there when you’re ready.
Prehab works. Four to eight weeks of progressive strengthening, aerobic conditioning, and balance training before surgery will measurably improve your recovery. Show up as strong and as fit as you can.
Protein intake matters before and after surgery. Aim for 1.2 to 1.6 g/kg/day, distributed across meals, with 30 to 40 grams per meal. Your body needs raw materials to heal.
Talk to your anesthesiologist about your medications, especially GLP-1 agonists, SGLT2 inhibitors, and blood thinners. Hold times and risks vary, and these conversations need to happen weeks before surgery, not the morning of.
Stop smoking. Reduce alcohol. Optimize your vitamin D. Correct anemia. These are not optional extras. They directly affect complication rates and healing.
Set realistic expectations. Recovery is measured in weeks and months, not days. The operation is the beginning of the process, not the end.
Don’t stop moving while you wait for surgery. Every day before the operation is a chance to get stronger. Use it.
For Members, below is a downloadable guide you can keep handy or share with friends and family preparing for elective surgery. Some surgeons’ offices and some surgery centers may follow different protocols regarding medications to take or avoid. Be sure to check with them.
